Be an Ocular Foreign Body Fixer
You have the tools and the knowledge to be your community’s ocular foreign body expert. Here’s how to incorporate these skills into your practice.
By Caroline B. Pate, OD
Release Date: April 15, 2019
Expiration Date: April 15, 2022
Estimated Time to Complete Activity: 2 hours
 |
Jointly provided by Postgraduate Institute for Medicine (PIM) and Review Education Group
Educational Objectives: After completing this activity, the participant should be better able to:
- Prioritize patients with ocular foreign bodies and know the important questions to ask during a detailed history.
- Perform careful ocular examination including pertinent testing and imaging, if needed.
- Provide anesthesia and remove various foreign bodies (metallic, vegetative, stone, insect) using the proper instrument and approach.
- Administer and/or prescribe antibiotics, corticosteroids or cycloplegia as appropriate.
- Describe when and where to refer patients whose injury is beyond the scope of the primary care optometrist.
- Provide appropriate follow-up and offer patient education regarding safety practices and eye protection.
Target Audience: This activity is intended for optometrists engaged in the care of patients with ocular foreign bodies.
Accreditation Statement: In support of improving patient care, this activity has been planned and implemented by the Postgraduate Institute for Medicine and Review Education Group. Postgraduate Institute for Medicine is jointly accredited by the Accreditation Council for Continuing Medical Education, the Accreditation Council for Pharmacy Education, and the American Nurses Credentialing Center, to provide continuing education for the healthcare team. Postgraduate Institute for Medicine is accredited by COPE to provide continuing education to optometrists.
Faculty/Editorial Board: Caroline B. Pate, OD, University of Alabama at Birmingham School of Optometry.
Credit Statement: This course is COPE approved for 2 hours of CE credit. Course ID is 62001-AS. Check with your local state licensing board to see if this counts toward your CE requirement for relicensure.
Disclosure Statements:
Dr. Pate has nothing to disclose.
Managers and Editorial Staff: The PIM planners and managers have nothing to disclose. The Review Education Group planners, managers and editorial staff have nothing to disclose.
Ocular foreign bodies typically arise following an acute injury to the eye. When this occurs, patients often report directly to the emergency department, even though optometrists have the tools and ability to medically manage many of these emergent cases.
The Centers for Disease Control and Prevention (CDC) estimates that more than 2.4 million emergency department visits each year are for eye-related trauma or disorders.1 Of the emergency department visits related to eye trauma, ocular foreign bodies account for an estimated 24% of cases. The majority of these cases are men of working age.1
 |
| Fig. 1. Using a lid retractor, double evert the lid to check the superior fornix. Click image to enlarge. |
Optometrists should be proactive in educating their patients regarding what to do in the case of an ocular emergency such as a foreign body. In addition, ODs should make sure their office staff is properly trained to identify and triage these emergency patients.
History is Key
While the diagnosis of an ocular foreign body is often fairly easy to make, be sure to start with a thorough problem-focused case history. Symptoms typically include foreign body sensation, redness, pain, irritation, tearing, photophobia, blepharospasm and possible blurred vision, depending on the location of the foreign body.2
The nature of the injury, suspected material involved and timing are all important to discuss and document in the medical record. The context of the injury is important to help identify if the foreign body was projectile in nature (e.g., grinding or metal striking metal), thus raising your suspicion for an intraocular foreign body and the potential need for further imaging.
Having an idea of what the foreign material may be can help identify the risk of potential complications and may influence your management options. Foreign bodies of organic (e.g., insect parts or animal hairs) or vegetative material are associated with a higher rate of infection.2-3 Inert foreign bodies such as glass or high-grade plastic are generally better tolerated and do not cause as much of an inflammatory response.4
Determine, as best as you can, how long the suspected foreign body has been present because duration can increase the risk of associated inflammation, infection and rust.2-5
Be sure to document the place and activity of the injury as well as whether or not the patient was wearing safety eye wear at the time of the injury, which can be important for liability issues such as worker’s compensation claims.
Ocular Examination
After a detailed history, obtain visual acuity before performing any procedures or instilling drops. If the patient is in significant discomfort and unable to open their eye due to intense blepharospasm or pain, a drop of topical anesthetic such as proparacaine may be instilled prior to visual acuity measurements. Preliminary testing should include pupil evaluation and extraocular motility.
 |
| Fig. 2. Everting the lids can reveal a conjunctival foreign body. Click image to enlarge. |
Foreign bodies can involve any part of the globe, so thoroughly evaluate both eyes for conjunctival, corneal and intraocular foreign bodies. It’s common for patients to have more than one foreign body depending on the nature of the incident. In any case of suspected ocular foreign body, always evert the eyelids.
For a more thorough evaluation of the superior fornix, double lid eversion can be accomplished using a lid retractor (Figure 1). Following a drop of topical anesthetic, single lid eversion is performed on the upper lid. Then use the lid retractor to “hook” the superior edge of the everted lid and lift gently upward and outward to expose the superior fornix. The superior fornix may then be directly visualized outside the slit lamp to further evaluate for foreign bodies or to perform conjunctival irrigation to help dislodge any debris that may be trapped. An external light source may be needed for better visualization.
Carefully examine the anterior segment, including the cornea and conjunctiva, using the slit lamp to evaluate for the presence of foreign bodies. If the foreign body involves the cornea, diffuse edema and epithelial disruption may be present. Instill fluorescein dye (preferably without anesthetic) to evaluate for evidence of epithelial defects. Multiple vertically oriented linear abrasions should raise suspicion for an embedded foreign body under the upper lid.
To assess for the presence of a full-thickness defect of the globe, perform a Seidel test by painting the wound with fluorescein dye and observing for aqueous leakage, which appears as a “dark waterfall” with the cobalt blue filter.
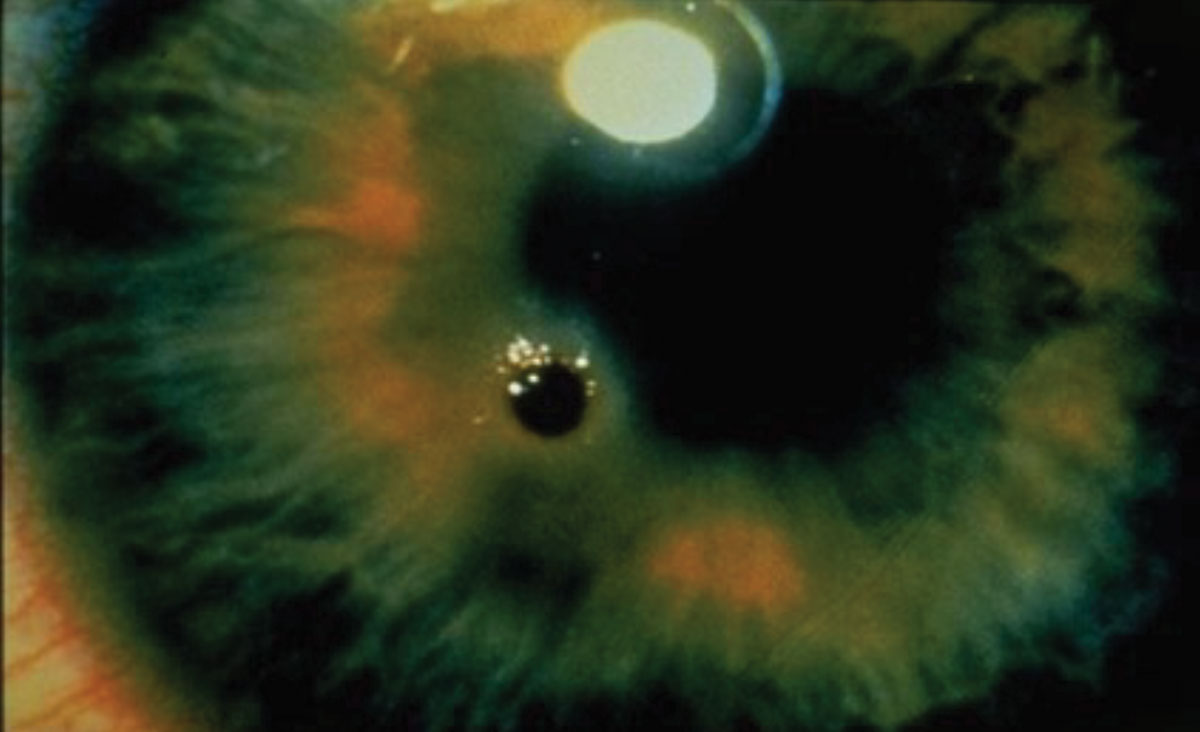
Apart from evidence of a ruptured globe with a positive Seidel sign or shallow anterior chamber, suspect intraocular foreign bodies in cases with an irregular pupil contour, iris transillumination defects, lens opacities or a persistent iritis.6-7
It’s possible for small foreign bodies to enter the globe and then have a self-sealing entry point due to the heat of a penetrating injury.7 Sometimes patients with intraocular foreign bodies present with a vague history of something getting in their eye but have no obvious external changes, so they initially dismiss the incident.
 |
| Fig. 3. Check for rust after removing a metallic corneal foreign body. Click image to enlarge. |
Intraocular foreign bodies can enter through the cornea (65%), sclera (25%) or at the limbus (10%).6,8 Most end up in the posterior segment (58% to 88%), while the remainder stay in the anterior chamber (10% to 15%) or lens (2% to 8%).4,6,9-11
Dilate the pupil and examine the posterior segment to further evaluate for penetrating foreign bodies, especially in cases with a projectile etiology such as hammering metal on metal or grinding.
Imaging may be necessary to further evaluate for intraocular foreign bodies. X-ray or computed tomography (CT) scans of the orbits with 1.0mm to 1.5mm axial and coronal cuts can help detect and localize intraocular foreign bodies when suspected.3,12 Magnetic resonance imaging is contraindicated in cases of metallic foreign bodies. With penetrating injuries, the globe should be stabilized and shielded without pressure, and the patient referred urgently to a specialist for management. Instruct the patient to avoid any food or drink as they may need to undergo same-day surgery to remove the intraocular foreign body. If not addressed urgently, complications such as traumatic endophthalmitis or metallosis may result.
If the foreign body involves the cornea, assess the location in relation to the visual axis and depth of the penetration using a thin optic section beam and document it in the medical record. Superficial corneal foreign bodies typically don’t penetrate past Bowman’s membrane, the tough layer that separates the epithelium and stroma.13 Superficial injuries to the corneal epithelium typically heal quickly within 24 to 48 hours without residual scarring.13,14
Table 1. Have These Tools Handy
|
When the corneal foreign body does penetrate beyond Bowman’s membrane, it disrupts layers of the cornea that have no mechanism to replace damaged cells and will likely leave a permanent scar.13 When it’s difficult to assess the level of corneal penetration, an anterior segment optical coherence tomography of the cornea may be helpful.
Ocular Foreign Body Removal
Prior to removing an ocular foreign body of the cornea or conjunctiva, obtain a signed informed consent form from the patient giving permission to perform the procedure to remove the foreign body. Informed consent involves discussing the nature of the condition, the proposed procedure, any risks associated with the procedure (which may include potential scarring, infection, vision loss or perforation), the alternatives to the procedure and the prognosis or consequence if the procedure is not performed.15 Always take time to address and answer any questions the patient may have before proceeding.
• Conjunctiva. Be sure to examine both the bulbar and palpebral conjunctiva thoroughly, including everting the upper lids, for the presence of suspected foreign bodies (Figure 2). After assessing the number, location and depth of the conjunctival foreign bodies, removal can be accomplished using irrigation, a sterile cotton-tipped applicator, spud, sterile disposable needle or jeweler’s forceps after topical anesthesia (Table 1).
If the foreign body is relatively superficial, the simplest method of removal is attempting to forcefully irrigate the eye so that it dislodges the foreign body, which can then be easily removed with a moistened cotton-tipped applicator or jeweler’s forceps. For foreign bodies that aren’t easily dislodged by irrigation or by swabbing the eye with a cotton-tipped applicator, try using a spud or sterile disposable needle. Inform the patient that a small subconjunctival hemorrhage may result following removal of a bulbar conjunctival foreign body.16
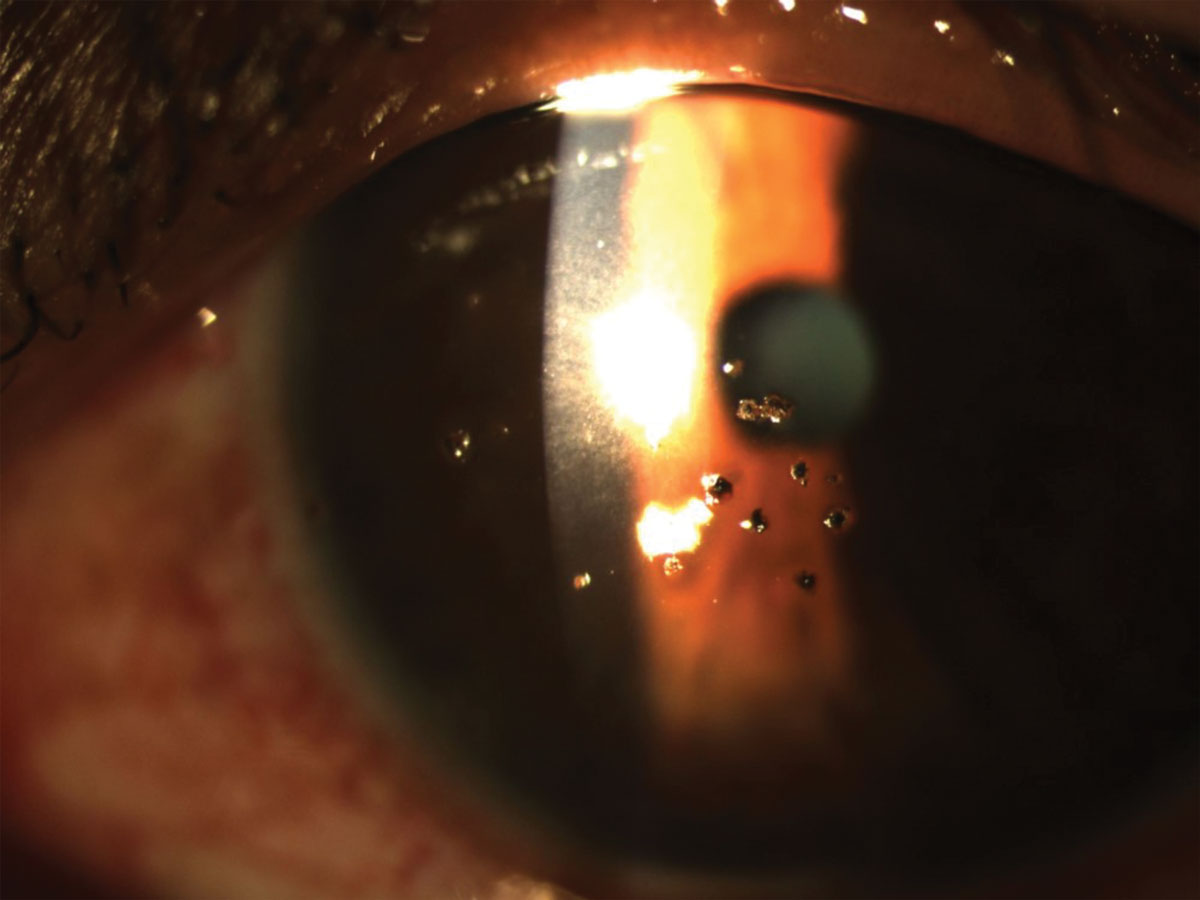
| Case Report: Follow Directions for Proper Eye Protection A 54-year-old African American male presented with bilateral painful red eyes for nine days. The patient reported a leak in a ventilation pipe at his place of employment (a pipe fabrication plant) that he walked by daily and felt he may have gotten debris in his eyes. He denied any grinding activities or striking metal on metal. He was wearing his glasses at the time of the injury but was not wearing the required safety glasses over his habitual correction as required by his employer. His current medical history was remarkable for Type 2 diabetes, hypertension and high cholesterol, all of which were currently managed with medications. Best-corrected visual acuity was 20/30+2 OD and 20/30 OS. Pupils were reactive with no afferent pupillary defect. Extraocular motilities were full with no restrictions. Slit lamp examination revealed 2+ injection of the bulbar conjunctiva OD and 3+ injection OS. The upper eyelids were everted and no foreign bodies were observed. One corneal metallic foreign body was noted OD and multiple diffuse metallic corneal foreign bodies were noted OS with associated corneal edema and epithelial defects. Seidel testing was negative. The irises were intact in both eyes.
After obtaining informed consent, proparacaine 0.5% was instilled in both eyes. The metallic foreign bodies were removed behind the slit lamp with a spud, and an Algerbrush was used to remove a small amount of residual rust from the left eye. Then the fornices were irrigated to remove any residual debris. The patient was dilated and no further intraocular foreign bodies were noted. A bandage contact lens was placed onto the left eye and the patient was prescribed topical moxifloxacin 0.5% TID and nepafenac 0.1% TID OU in addition to preservative-free artificial tears for comfort. The patient was counseled on the importance of proper eye protection while at work and instructed to return to the office for follow up in 24 hours. In addition, due to the clinical presentation of multiple foreign bodies and nature of the injury, an X-ray of the orbits was ordered to rule out intraocular foreign bodies, which was negative. This case demonstrates that although the patient was wearing glasses at the time of injury, they were inadequate for preventing material from entering in from the sides of his eyewear. As a result of not wearing the fit-over safety eye protection as required by his workplace, the patient proceeded to return on three additional occasions with similar presentations, despite being educated at each visit on the importance of proper eye protection. The patient’s employer was notified regarding the multiple occurrences. |
• Cornea. Foreign bodies lodged here can be removed using a variety of instruments, including a small-gauge disposable needle, a foreign body spud or a loop. Sterile disposable needles come in a variety of diameters (gauges) and lengths—the 25-gauge 5/8-inch size needle is popular for corneal foreign body removal due to its short length and minimal flexure. A foreign body spud, often referred to as a golf club spud due to its characteristic shape, allows the clinician to excavate and gently “flick” the foreign body off of the cornea. The dislodged foreign body can then be retrieved using jeweler’s forceps. Magnetic spuds help gently lift a metallic foreign body off the cornea and then easily retrieve it.
A foreign body loop can be used to remove loosely embedded corneal foreign bodies. Due to its flexibility, a loop can be quite helpful for children or uncooperative patients.
A sterile cotton-tipped applicator is not a good choice for an embedded corneal foreign body due to the bulkiness of the tip of the applicator, which may embed the foreign body further or cause unnecessary adjacent epithelial disruption.
For patients with a strong blink reflex despite instillation of bilateral topical anesthetic, a lid speculum may be required to move the lids out of the way.
Regardless of which instrument is used to remove the corneal foreign body, be sure to educate the patient about the importance of maintaining fixation throughout the procedure. To help the patient fixate using their opposite eye, put a fixation target from the slit lamp into place.
Once the patient is anesthetized and properly positioned behind the slit lamp, hold the instrument between your thumb and forefinger like a pencil and stabilize your hand against the patient’s cheek. Make sure to always approach the cornea tangentially to help avoid corneal perforation. While viewing outside of the slit lamp, bring the instrument towards the cornea until the instrument is positioned in front of the foreign body. Then move into position behind the slit lamp oculars to safely position the instrument at the temporal peripheral edge of the foreign body, where you can gently lift it off the cornea using a delicate flicking motion.
Once you’ve removed a metallic foreign body, examine the cornea for the presence of any rust (Figure 3). After the metal has been in the cornea for approximately 12 hours, it will start to oxidize and form a rust ring in adjacent tissues.5,16
You may be able to remove some rust with a disposable needle or the jeweler’s forceps and then use a low-speed motorized burr (Algerbrush) to remove the remaining rust. The 0.5mm burr is preferred for rust ring removal and should be properly disinfected prior to its use. Disposable dental burrs are also available.
Inform the patient of the procedure and, if necessary, demonstrate the slight buzzing sound that they may hear from the motorized burr. Approach the cornea tangentially with the Algerbrush as the burr head rotates on the cornea to remove the rust ring. Some pressure should be applied during the procedure, keeping in mind that the battery-powered Algerbrush has a built-in mechanism to stop rotating when a certain amount of resistance is encountered—this helps to prevent the instrument from penetrating Bowman’s membrane.16
| Billing and Coding for Ocular Foreign Bodies CPT Considerations An office visit is already included in the surgical procedure code, and an exam code should not be billed in addition to the 652XX code. In addition, a bandage contact lens fit is not allowed to be billed on the same day as the minor corneal surgical procedure. The one exception to this would be if you discover another problem that is unrelated to the minor surgical procedure that needs to be addressed during the same office visit, in which a -25 modifier would be used with the appropriate 99XXX E/M code.
The above CPT codes are bundled codes. This means that if there are two or more foreign bodies in the same tissue in the same eye, only one code for the procedure can be billed, no matter how many foreign bodies you remove. But, if the patient has foreign bodies in both the cornea and conjunctiva of the same eye, you can report both 65210 and 65222 separately (with modifier -51). If the patient has foreign bodies in two separate eyes, you can report the same code with the –RT and –LT modifiers separately; however, many carriers will adjust the reimbursement for bilateral procedures on the same day. The global period associated with these procedures is zero days. ICD-10 Options
Many carriers are not yet requiring the W or Y ICD-10 codes; however, we should become accustomed to using them as they may be required in the future. Upon follow-up the next day for the above example, a 992XX office visit would now be the appropriate choice, along with T15.02XD, with the “D” indicating a subsequent encounter if the patient is not under active management, for which you would continue to use the “A” in the seventh position. Only when the patient is not being actively managed do you change the diagnosis to the “D” or subsequent visit status. Sequela, indicated by an “S” in the seventh position, is used for complications or conditions that arise as a direct result of the condition. | ||||||||||||
Following the procedure, a small crater-like epithelial defect will remain. In the event that residual rust remains or the risk of the procedure prohibits full removal of remaining rust, any residual rust will eventually dissipate or rise to the epithelial surface during the healing process, and you can remove it at a later time or leave it in place if it’s not impeding the healing process.7,13,17 Residual rust may also create additional inflammation and slow the healing process, so try to remove as much of the rust as possible.5
According to CDC recommendations, any reusable equipment used during the process of conjunctival or corneal foreign body removal should be thoroughly disinfected. This can be accomplished using a 15-minute soak in 1:10 diluted bleach or a 20-minute soak in 2% glutaradehyde.18,19 You can also use an autoclave to sterilize your instruments.
Management and Follow Up
Following corneal foreign body removal, a residual epithelial defect may remain with surrounding corneal edema and conjunctival injection. Depending on the amount of time the foreign body was in the eye, a secondary anterior uveitis may also occur. This should resolve with the appropriate treatment as the cornea heals. Manage the patient in the same way you would treat a patient with a corneal abrasion.
Postoperative management for both conjunctival and corneal foreign body removal should include placing the patient on a topical broad-spectrum antibiotic for one week to help prevent infection. Pain management is patient specific and often depends on the extent and depth of the residual corneal defect. Topical or systemic therapy may be initiated. Cycloplegia with 1% cyclopentolate or 5% homatropine BID to TID not only assists with ocular pain from ciliary spasm, but also helps decrease the secondary iritis that can accompany the trauma. Topical ophthalmic non-steroidal anti-inflammatory agents can assist in pain control, although they may delay the healing process.20
In cases with a residual defect or significant pain, consider a bandage contact lens to promote healing while decreasing the risk of future recurrent corneal erosions. Keep in mind that bandage contact lenses should not be used in cases with an organic etiology. Pressure patching is often unnecessary.21 Preservative-free artificial tears during the day and topical ointment at bedtime can aid in patient comfort and assist in lubricating the cornea during healing.
Follow these patients every 24 hours until the cornea shows improvement and a restored epithelium. Once the cornea has re-epithelialized, a topical steroid (alone or a combination antibiotic-steroid) can be added to reduce inflammation, scarring and the risk of subepithelial infiltration. In cases of organic corneal foreign bodies, wait until the cornea shows healing before employing steroids due to the risk of potentiating infection.7 Consider placing an amniotic membrane for severe, central or deep corneal defects that have the greatest risk for scarring and reduced vision.
Remind patients during their annual visits that you are available and equipped to handle eye emergencies, and they’re welcome to reach you should they have an after-hours eye emergency. Make a point to understand your patient’s day-to-day activities, including their occupation and hobbies and any safety risks they may encounter. By being proactive, you can help reduce the costly, and often unnecessary, emergency room visits related to eye emergencies, including ocular foreign bodies. Finally, emphasize to your patients the importance of safety practices and proper eye protection for the prevention of future ocular foreign body episodes.
Dr. Pate is an associate professor at the University of Alabama at Birmingham School of Optometry.
|
1. Haring RS, Canner JK, Haider AH, Schneider EB. Ocular injury in the United States: Emergency department visits from 2006-2011. Injury. 2016;47(1):104-8. 2. Fraenkel A, Lee LR, Lee GA. Managing corneal foreign bodies in office-based general practice. Aust Fam Physician. 2017;46(3):89-93. 3. Bowling B, Kanski JJ. Kanski’s Clinical Ophthalmology: A Systematic Approach. 8th ed. Edinburgh: Elsevier; 2016:878-81. 4. Upshaw JE, Brenkert TE, Losek JD. Ocular foreign bodies in children. Pediatr Emerg Care. 2008;24(6):409-14. 5. Shetler J, Lighthizer N. Foreign body removal in 12 steps. Rev Optometry. 2015;152(1):22-9. 6. Loporchio D, Mukkamala L, Gorukanti K, et al. Intraocular foreign bodies: a review. Surv Ophthalmol. 2016;61(5):582-96. 7. Bronner A. No insult to injury: managing foreign body removal. Rev Optometry. 2017;154(1):47-54. 8. Rathod R, Mieler WF. An update on the management of intraocular foreign bodies. Retin Physician. 2011;8(3):52-5. 9. Jonas JB, Knorr HL, Budde WM. Prognostic factors in ocular injuries caused by intraocular or retrobulbar foreign bodies. Ophthalmology. 2000;107(5):823-8. 10. Katz G, Moisseiev J. Posterior segment intraocular foreign bodies: an update on management. Retin Physician. 2009;6(3):32-4. 11. Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in China: clinical characteristics, prognostic factors, and visual outcomes in 1,421 eyes. Am J Ophthalmol. 2011;152(1):66-73.e1. 12. Nie S, Wang Z, Liu W, Liang X. Clinical application of X-ray, B-scan, and CT in the diagnosis of ocular foreign bodies. Eye Sci. 2013;28(1):11-4. 13. Gurwood AS. That’s gonna leave a mark. Rev Optometry. 2017;154(8):98. 14. Leinert J, Griffin R, Blackburn J, McGwin G Jr. The epidemiology of lawn trimmer injuries in the United States: 2000-2009. J Safety Res. 2012;43(2):137-9. 15. Eftekhari K, Binenbaum G, Jensen AK, et al. Confidence of ophthalmology residents in obtaining informed consent. J Cataract Refract Surg. 2015;41(1):217-21. 16. Casser L, Fingeret M, Woodcome HT. Atlas of Primary Eyecare Procedures. 2nd ed. New York; McGraw Hill; 1997:156-9, 170-3. 17. Crowther KS, Ellingham RB. Complicated removal of corneal foreign bodies 18 months after laser in situ keratomileusis. J Cataract Refract Surg. 2005;31(4):851-2. 18. Tyhurst KN, Hettler DL. Infection control guidelines – an update for the optometric practice. Optometry. 2009;80(11):613-20. 19. Rutala WA, Weber DJ. Guideline for disinfection and sterilization in healthcare facilities, 2008. Centers for Disease Control and Prevention. www.cdc.gov/infectioncontrol/guidelines/disinfection. Accessed January 19, 2019. 20. Weaver CS, Terrell KM. Evidence-based emergency medicine. Update: do ophthalmic nonsteroidal anti-inflammatory drugs reduce the pain associated with simple corneal abrasion without delaying healing? Ann Emerg Med. 2003;41(1):134-40. 21. Menghini M, Knecht PB, Kaufmann C, et al. Treatment of traumatic corneal abrasions: a three-arm, prospective, randomized study. Ophthalmic Res. 2013;50(1):13-8. |