Uncover the symptoms of this deadly condition and know how to help manage the patient.
By Trenton Cleghern, OD
Release Date: September 15, 2018
Expiration Date: August 23, 2021
Goal Statement: Giant cell arteritis is a rare, but urgent and potentially life-threatening, presentation that can have ocular consequences. This course details how to tell which patients are likely to have it based on their history and symptoms as well as how to test for it using both imaging and lab work, and reviews the optometrist’s role in treating and comanaging these patients. It also details likely comorbidities.
Faculty/Editorial Board: Trenton Cleghern, OD
Credit Statement: This course is COPE approved for 2 hours of CE credit. Course ID is 59140-NO. Check with your local state licensing board to see if this counts toward your CE requirement for relicensure.
Disclosure Statements:
Authors: The author has no relationships to disclose.
Editorial staff: Jack Persico, Rebecca Hepp, William Kekevian, Catherine Manthorp and Mark De Leon all have no relationships to disclose.
Giant cell, temporal or cranial arteritis is a systemic vasculitis involving mainly the medium-to-large arteries of the head and neck. The condition can affect blood vessels elsewhere in the body, but tends to involve the cranial and ophthalmic arteries. Giant cell arteritis (GCA) is an autoimmune condition of unknown etiology. It is the most common systemic vasculitis seen in adults.1 GCA occurs in adults older than 70 and has a wide variety of symptoms and complications.2 It is of particular interest to eye care providers due to its potential for visually devastating complications, such as rapidly progressing bilateral blindness.
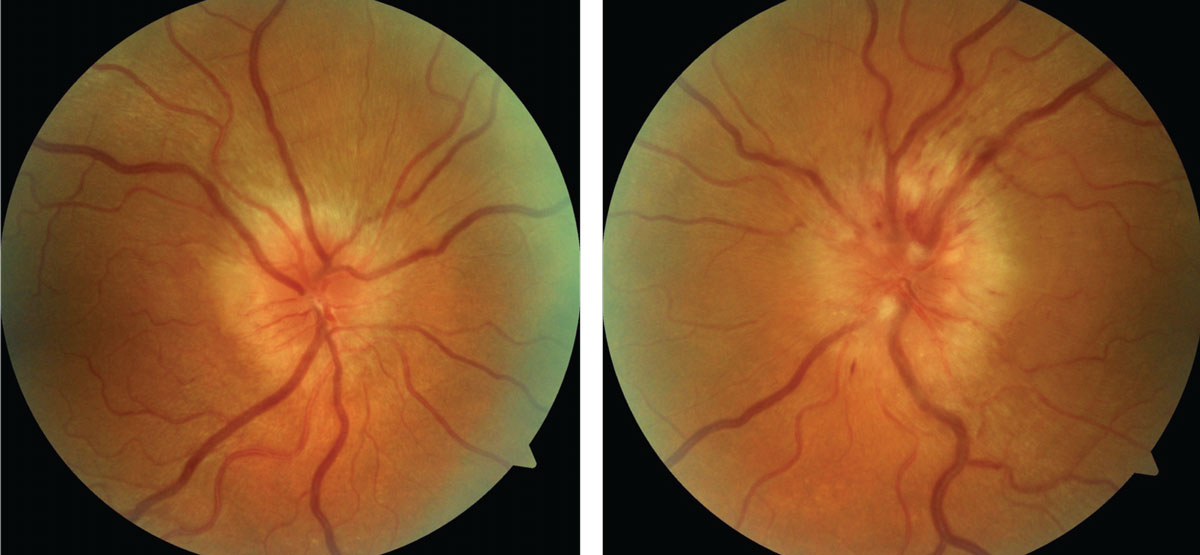 |
| Optic nerve photos of a 65-year-old Caucasian patient with bilateral disc edema, headache and scalp tenderness. Presentations such as this warrant immediate steroid therapy and blood work. Click image to enlarge. |
Temporal arteritis is a topic that is introduced as early as the first or second year in an optometric curriculum because of its dire, and potentially deadly, consequences. The condition can present in a variety of ways, making diagnosis a challenge. Patients may present with only systemic symptoms, or only ocular symptoms. This article focuses on the clinical presentation of GCA. This condition can simply never be missed—for the sake of the patient’s vision and life.
The Basics
We know that GCA is a condition of older adults and that it is extremely rare to occur before age 50.2 Research places the average age of diagnosis approximately 72 to 77 years.2 Age is actually the greatest risk factor, though the risk does rise after age 50.2 Similar to other autoimmune disease, the risk of developing GCA is more common in women, with a ratio of three to one, women to men.7 Temporal arteritis is also more common in Caucasian individuals, especially those from Scandinavian countries or of Scandinavian descent. The disease is rare in black and Asian populations. It was once thought to be rare in Hispanic populations, but some recent evidence has questioned that notion.3
GCA is a systemic autoimmune vasculitis with an unknown origin. It is typically a medium and large vessel disease, but may also affect small vessels. When larger vessels, such as the carotid, subclavian or aorta are affected, it is referred to as large-vessel GCA.4 Immune cells made of mostly T-lymphocytes and macrophages invade the arterial wall.5 Granulomatous changes can then occur, leading to the formation of giant cells. This causes vascular remodeling of the inner vessel wall in the form of hyperplasia. The remodeled lumen can become occluded, which is the cause of the ischemic events in GCA. The disease process likely occurs from an inciting event in a susceptible individual.
Table 1. Most Commonly Reported Symptoms in GCA | ||
| Symptom | Initial | Throughout Course of Disease |
| Headache | 33% | 72% |
| Neck/torso/pelvic pain | 25% | 58% |
| Fatigue and malaise | 20% | 56% |
| Jaw claudication | 4% | 40% |
| Fever | 11% | 35% |
| Seetharaman M. Giant Cell Arteritis (Tempeoral Arteritis) Clinical Presentation. Medscape. emedicine.medscape.com/article/332483-clinical. | ||
Many environmental and microbial origins have been proposed, including the herpes zoster viruses, but none have been found to have a causal relationship.6,7
Patients with GCA can present with a variety of symptoms, creating a diagnostic challenge. Patients may present to an eye care provider with only vision complaints, or may present to a general practitioner with only systemic complaints. Of course, the patient may have both ocular and systemic complaints. The patient’s symptoms can either be acute or subacute, but tend to be more subacute.7 The most common systemic symptoms in GCA are headache, scalp tenderness, neck/shoulder/pelvic pain, fatigue, malaise, weight loss, jaw claudication and fever (Table 1).8
Systemic Symptoms
Headache is the most common symptom in GCA.8 No pathognomonic features are associated with the headache in GCA, except that the complaint is new. If a patient has chronic headaches, the patient would describe a new type of headache. The pain is usually temporal, occipital or diffuse. Headaches are usually constant in GCA patients, but may wax and wane. Patients may describe the headache as throbbing, boring, dull or even burning.
Even though headache is the most common symptom, patients need to be specifically questioned because they may not associate the headache with other symptoms.8 The headache should resolve rapidly after the institution of oral or intravenous steroids. When the headache does not resolve after initial steroid treatment, other etiologies must be investigated.
Scalp tenderness is sometimes included as part of the headache complaint. However, its presence can indicate an inflamed superficial temporal artery. Even light touches, such as brushing one’s hair or putting on spectacles, can elicit pain over this area. The superficial temporal artery should be palpated in patients in whom you have suspicion for temporal arteritis, even if the patient makes no complaint of scalp tenderness.
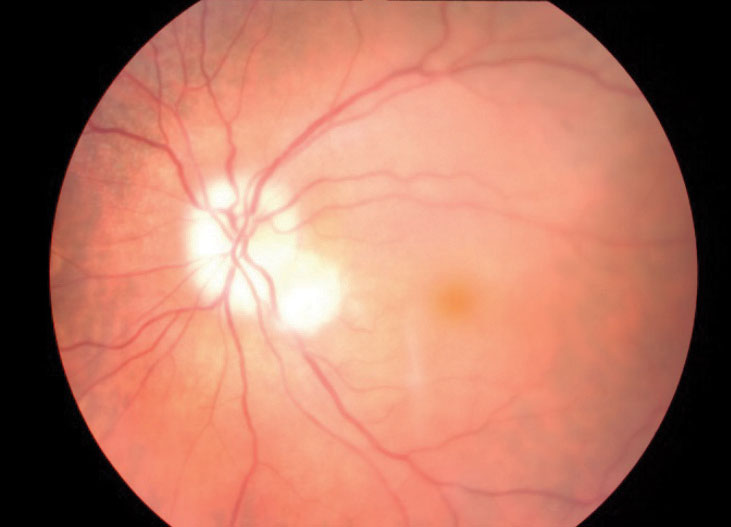 |
| This optic nerve image shows retinal ischemia consistent with AAION, the most common cause of vision loss from GCA. Photo: Steven Bloom, MD |
GCA patients may also complain of neck, shoulder, torso or hip girdle pain. Affected patients may have fatigue, weight loss or malaise. Constitutionally, they will seem very poor in most cases. Generally, GCA patients look and feel very ill. In my experience, it’s unlikely these patients will sit in your exam chair with a cheerful disposition. Jaw claudication, or pain after prolonged chewing, is a result of ischemia of the maxillary artery, which provides blood flow to the masseter muscles in the jaw. Jaw or tongue claudication, visual abnormalities and temporal artery abnormalities are the highest specific clinical features. When compared with other symptoms, jaw claudication had the highest association with a positive temporal artery biopsy.9 Patients need to be specifically questioned about jaw claudication, because again they might not associate their jaw symptoms with their presenting complaint.
Fever is a non-specific symptom that GCA patients will sometimes experience. Interestingly, one study found that one in six fevers in older adults with an unknown etiology were from temporal arteritis.10
Other, less common systemic symptoms include: maxillary pain, facial swelling, tongue or throat pain, dysarthria, hearing loss, limb claudication, stroke, carpel tunnel syndrome and pericarditis.7,11 In large-vessel GCA, aortitis, aortic dissection and aortic aneurysm are possible complications. Large artery GCA, compared with cranial arteritis, tends to affect patients at a younger age, produce fewer headache symptoms and are less likely to have a positive temporal artery biopsy.12
Table 2. Erythrocyte Sedimentation Rate Norms | |
| Men | Women |
| Age/2 | (Age + 10)/2 |
| Younger than age 50: less than 15mm/hour | Younger than age 50: less than 20mm/hour |
| Older than age 50: less than 20 mm/hour | Older than age 50: less than 30mm/hour |
Ocular Symptoms
Approximately half of GCA patients experience visual symptoms over the course of the condition.13 Vision loss can be transient or constant, unilateral or bilateral. The vision loss is usually painless, although the patient may complain of pain elsewhere, such as headache, scalp tenderness or other body aches. Patients may have actual ocular pain as well from associated ocular ischemia. The patient may experience transient vision loss. Sudden, persistent loss of vision is often irreversible. Vision loss in the fellow eye can occur in a significant portion of patients.13 The second eye can become involved in one to two weeks, but it can happen sooner.6 Once corticosteroid therapy has been initiated, new or further vision loss is fairly rare.
The most common cause of vision loss in GCA is from arteritis anterior ischemic optic neuropathy (AAION) at around 80% of cases.6 AAION is the result of vessel occlusion of the short posterior ciliary arteries or ophthalmic artery. Other causes of vision loss include central retinal artery occlusion (CRAO), branch retinal artery occlusion (BRAO), posterior ischemic optic neuropathy (PION) and cerebral ischemia. CRAO accounts for about 10% of vision loss in GCA.6 If a patient at least 55 years of age presents with bilateral CRAO, or unilateral CRAO with no vascular risk factors, a GCA investigation should be included in the work-up. BRAO and PION are rare causes of vision loss in GCA.6 Cerebral ischemia from GCA occurs because of infarction in the vertebrobasilar circulation.
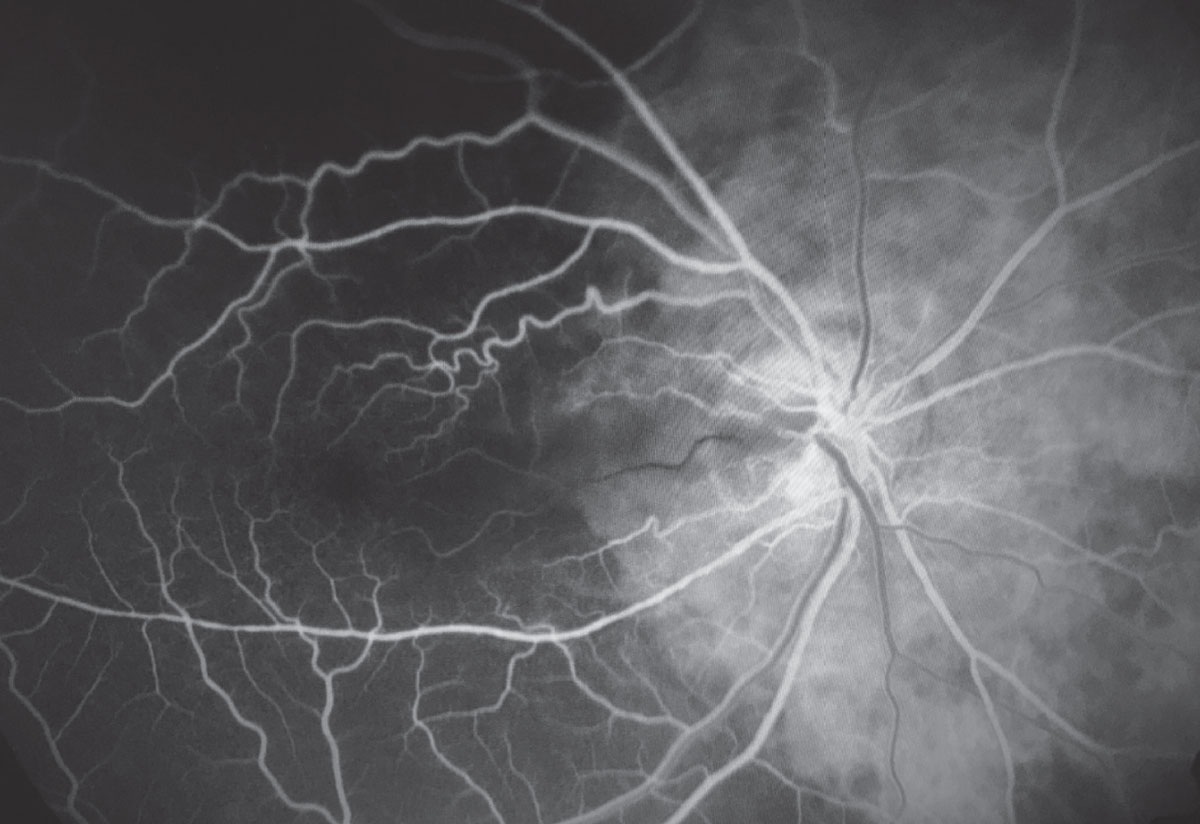 |
| This fluorescein angiography of a GCA patient shows choroidal ischemia temporally, optic nerve leakage and cilioretinal artery occlusion. Photo: Kristin Madonia, MD. Click image to enlarge. |
Another symptom of temporal arteritis patients, although rare, is diplopia. About 5% of patients may have diplopia from either sixth or third nerve palsies.13 Sixth nerve palsy with GCA is slightly more common than third nerve.13 This occurs from ischemia to either the muscles, cranial nerves or even the brain stem. When encountering an older patient with an isolated sixth or third nerve palsy, inquire about GCA-related symptoms.
Clinical Evaluation
GCA patients can present clinically in a variety of scenarios. The clinician must be able to perform a thorough and detailed examination if temporal arteritis is suspected. Reduced acuity is a concerning finding because of the high likelihood of permanent vision loss.5 The extraocular motilities and cover test must be performed to evaluate for a sixth or third nerve palsy. This is a rare finding, but isolated cranial nerve palsies without any other ophthalmic signs of GCA have been reported.7 Pupil assessment is paramount to look for a relative afferent pupillary defect (RAPD). If both nerves are affected, there may not be an RAPD. In this scenario, the pupils may be sluggish to react to light depending on the optic nerve involvement. Color vision may affected due to the damaged optic nerves, so this should be included in the work-up.
Visual fields, optical coherence tomography (OCT) and fundus photos are helpful to obtain during the evaluation. Visual field defects in GCA can vary and could be altitudinal, diffuse or enlarged blind spots. It is imperative to obtain a visual field to assess for any field loss, and to have as a baseline. When optic nerve edema is present, OCT of the retinal nerve fiber layer is clinically useful to obtain objective data. It is easy to observe optic nerve edema using the slit lamp, but an OCT of the optic nerve provides a quantitative value to monitor for progression. As with visual fields and OCT, fundus photographs of the optic nerve and posterior pole should be obtained to monitor for progression.
| Examination Tips When an adult older than 55 presents with with optic nerve edema, question them thoroughly about systemic symptoms including headache, scalp tenderness, jaw claudication, aches, fatigue and fever. Never ignore headache complaints. Temporal arteritis patients may only experience systemic complaints, but ocular involvement can occur later. A laboratory work-up should be initiated as soon as possible. However, steroids should not be withheld to obtain laboratory tests beforehand. In these cases, always evaluate both eyes, even if the complaints are monocular. This goes without saying, but the appearance of the fellow optic nerve can be quite helpful in distinguishing non-arteritic AION from arteritic AION. |
Nearly all the ophthalmic findings in GCA are in the posterior segment; however, anterior segment ischemia can be present, as well as cells and flare in the anterior chamber. Ocular ischemic syndrome is a rare but documented sequela from GCA.13 If ocular ischemic syndrome is present, patients may manifest neovascularization of the iris, anterior chamber inflammation and elevated IOP.18 Potential posterior segment findings include optic disc edema, CRAO, retinal hemorrhages and cotton wool spots.17 The disc edema in AAION is sometimes described as “chalky white.”16 This term refers to the pallor that can happen quickly in the disease process, sometimes in as little as a few weeks. Cotton-wool spots may be present as a result of severe ischemia. Retinal hemorrhages associated with the disc edema typically emanate from the optic nerve in a radial pattern. If a CRAO is present with concurrent optic nerve edema, GCA is likely.
Lab Work
Blood testing plays a large role in the evaluation of patients suspected to have GCA. The two main lab tests to aid in the diagnosis are the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). A complete blood count (CBC) can also be extremely helpful. The hallmark laboratory finding in GCA is an elevated ESR and CRP.5Both the ESR and CRP are acute phase reactants that the body produces in reaction to infection or inflammation. The ESR is measured in millimeters per hour (mm/hour) and the CRP is measured in milligrams per liter (mg/L). Neither are specific to GCA, but when both are elevated, the sensitivity and specificity is greatly increased.
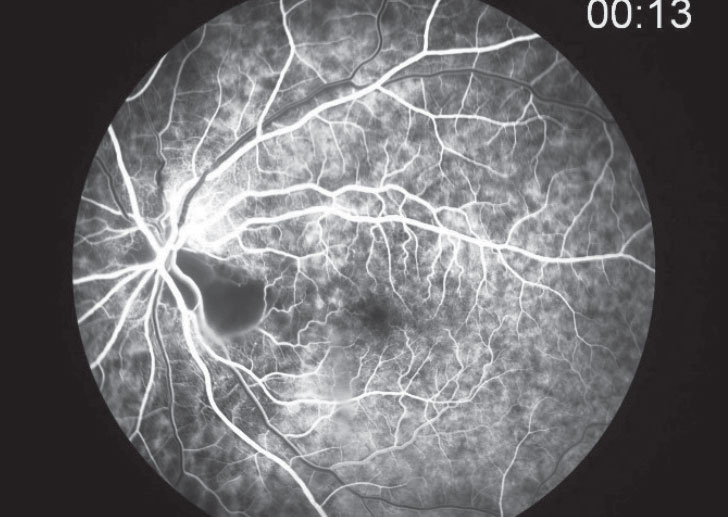 |
| Fluorescein angiography for GCA patients typically shows delayed choroidal and central retinal artery filling, with possible choroidal non-perfusion, especially in the peripapillary area. Photo: Steven Bloom, MD. |
A significant number of patients can have a positive temporal artery biopsy with a normal ESR and CRP.14 In a study of 167 biopsy-proven GCA patients, the ESR was less than 50mm/hour in 11% of patients and less than 40mm/hour in 5%.14 A normal ESR and CRP does not rule out GCA, but an elevated ESR and CRP raises the likelihood of having the condition. A CBC can reveal a normochromic normocytic anemia, as well as an elevated platelet count. The liver enzymes, alkaline phosphatase and aspartate aminotransferase can be elevated in some GCA patients, but are not routinely ordered in clinical practice.
ESR is age- and gender-dependent (Table 2). The CRP is not age or gender specific. A CRP under 10mg/L is considered normal.
Since GCA cannot be excluded based on a normal ESR and CRP, a temporal artery biopsy is necessary for diagnosis. This biopsy is standard for diagnosing GCA. Patients suspected of having GCA should be referred to a neuro-ophthalmologist or oculoplastic surgeon for a biopsy. If these disciplines are not available, facial plastic surgeons, vascular surgeons or neurosurgeons can perform the biopsy.
It is important to order the temporal artery biopsy because GCA requires prolonged treatment with oral corticosteroids or immunosuppressants for six to 18 months. Keep in mind, temporal artery biopsies can produce false negatives due to “skip lesions.” Therefore, a 1.5cm to 2cm biopsy should be obtained to avoid these skip areas of the artery. Another diagnostic option for GCA is color duplex ultrasonography (CDUS). Scanning the head, neck and upper extremities with CDUS is noninvasive and can provide information on arteries other than the temporal artery. However, at this time more research needs to be done to determine the effectiveness of CDUS, and thus temporal artery biopsy remains the standard.
| Polymyalgia Rheumatica This systemic autoimmune disease causes shoulder and hip girdle pain. About 50% of GCA patients also have polymyalgia rheumatica (PMR), and around 10% to 15% of PMR patients develop GCA.7 The epidemiology mirrors that of GCA. Controversy exists as to whether GCA and PMR are separate diseases or different manifestations on a spectrum of the same disease. PMR responds well to low-dose corticosteroids and a rapid response is considered pathognomonic. For patients who do not respond to steroids, another diagnosis should be considered. The prognosis is excellent, but relapses can happen if steroids are tapered too quickly. Any patient with PMR with complaints of loss of vision, headache, scalp tenderness, jaw claudication or fever need to be urgently investigated for GCA.
|
Long-term Management
When you have an older adult patient with suspicion of GCA, clinicians should not hesitate to start oral steroid therapy. A laboratory work-up should be initiated as soon as possible. However, steroids should not be withheld to obtain laboratory tests or temporal artery biopsy beforehand. At our clinic, we employ the “shoot first and ask questions later” philosophy with temporal arteritis. It is better to start oral steroid therapy and soon discover that is not GCA than to withhold steroids and have the patient suffer devastating vision loss. Of course, we are judicious to ascertain that GCA is a legitimate concern due to the serious adverse effects of oral steroid therapy. High-dose oral steroids can elicit significant side effects, but they are usually minimal during a short duration. In our practice, we typically prescribe 80mg of prednisone to be taken as four 20mg tablets in one dose. Steroid therapy can also be given intravenously followed by an oral taper.
In true temporal arteritis, patients will sometimes need steroid therapy for six to 18 months, so they are most appropriately managed by neuro-ophthalmology or rheumatology long-term. Somewhat recently, the immunosuppressant drug, Actemra (tociluzumab, Genentech), has emerged an option for GCA patients.14 In many cases, it is not ideal for patients to be on steroids for over a year, so that is where immunosuppressant drugs may play a future role in GCA treatment.
While GCA patients are best managed by neuro-ophthalmology or rheumatology, it is optometry’s responsibility as the primary eye care providers to recognize and treat these patients in the initial presentation of the condition. GCA suspects require a shoot-first-ask-questions-later approach. It is better to start oral steroid therapy and soon discover that is not GCA, than to withhold steroids and see patients suffer devastating vision loss.
Dr. Cleghern is a staff optometrist at VisionAmerica of Birmingham in Alabama and an assistant clinical professor at University of Alabama at Birmingham School of Optometry.
|
1. Kermani T, Schäfer VS, Crowson CS, et al. Increase in age at onset of giant cell arteritis: a population-based study. Ann Rheum Dis. 2010 Apr;69(4):780-1. 2. Biousse V, Newman NJ. Ischemic optic neuropathies. N Engl J Med. 2015;372(25):2428-36. 3. Cid M, Campo E, Ercilla G, et al. Immunohistochemical analysis of lymphoid and macrophage cell subsets and their immunologic activation markers in temporal arteritis. Influence of corticosteroid treatment. Arthritis Rheum. 1989;32(7):884-93. 4. Brack A, Martinez-Taboada V, Stanson A, et al. Disease pattern in cranial and large-vessel giant cell arteritis. Arthritis Rheum. 1999;42(2):311-7. 5. Gonzalez-Gay MA, Barros S, Lopez-Diaz MJ, et al. Giant cell arteritis: disease patterns of clinical presentation in a series of 240 patients. Medicine (Baltimore). 2005;84(5):269-76. 6. Seetharaman M. Giant cell arteritis (Temporal Arteritis) clinical presentation. Medscape. emedicine.medscape.com/article/332483-clinical-presentation. July 11, 2017. Accessed July 30, 2018. 7. Docken W, Rosenbaum J. Clinical manifestations of giant cell arteritis. www.uptodate.com/contents/clinical-manifestations-of-giant-cell-arteritis. December 8, 2017. Accessed July 30, 2018. 8. Gabriel S, O’Fallon W, Achkar A, et al. The use of clinical characteristics to predict the results of temporal artery biopsy among patients with suspected giant cell arteritis. J Rheumatol. 1995;22(1):93-6. 9. Knockaert D, Vanneste L, Bobbaers H. Fever of unknown origin in elderly patients. J Am Geriatrics Soc. 1993;41(11):1187-92. 10. Bhatti M, Frohman L, Nesher G. MD roundtable: diagnosing giant cell arteritis. EyeNet. 2017;21(6):31-4. 11. Waldman C, Waldman S, Waldman R. Giant cell arteritis. Med Clin North Am. 2013;97(2):329-35. 12. Salvarani C, Hunder G. Giant cell arteritis with low erythrocyte sedimentation rate: frequency of occurence in a population-based study. Arthritis Rheum. 2001;45(2):140-5. 13. Hayreh S, Podhajsky P, Zimmerman B. Ocular manifestations of giant cell arteritis. Am J Ophthalmol. 1998;125(4):509-20. 14. FDA approves Roche’s Actemra/RoActemra (tocilizumab) for giant cell arteritis. Roche. www.roche.com/media/releases/med-cor-2017-05-23.htm. May 23, 2017. Accessed July 30, 2018. |