Our understanding of dry eye disease (DED) has grown tremendously in recent years. As the prevalence of associated systemic conditions grows, optometrists must be aware of the connections between systemic conditions and DED.1,2 Autoimmune diseases such as Sjögren’s syndrome (SS), rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) are often linked to DED, for example.3,4 Diabetes mellitus (DM) also is an important systemic cause of dry eye.5 Consequently, both DM and SS are key systemic conditions clinicians should explore when examining DED patients. These clinical clues can help optometrists intervene sooner to provide the best management options.
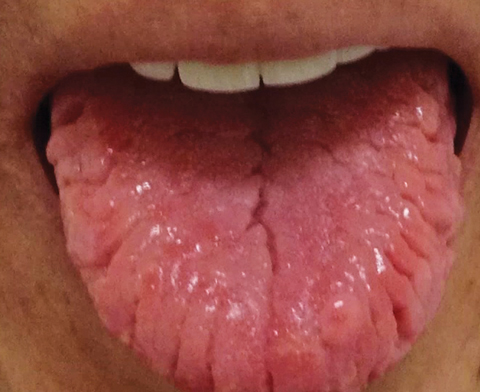 |
| A sore, cracked tongue is suggestive of Sjögren’s syndrome. Click photo to enlarge. |
Diabetes
Research suggests more than 50% of patients with DM have dry eye, and significant associations exist between DED and the duration of diabetes and diabetic retinopathy.6-9 Meibomian gland dysfunction (MGD) is also associated with DM, and one study shows a significant increase in the frequency of MGD in diabetes patients compared with those unaffected.10,11
Clinical clues. Polyuria and polydipsia are known symptoms of DM, and patients often report typical dry eye symptoms such as burning, foreign body and gritty sensations and sore eyes.6-8 However, practitioners should be mindful that patients with longstanding diabetes may report fewer symptoms as a result of diabetic corneal neuropathy.5 A closer examination is warranted in patients presumed to suffer from DED who present with insignificant symptoms or none at all.
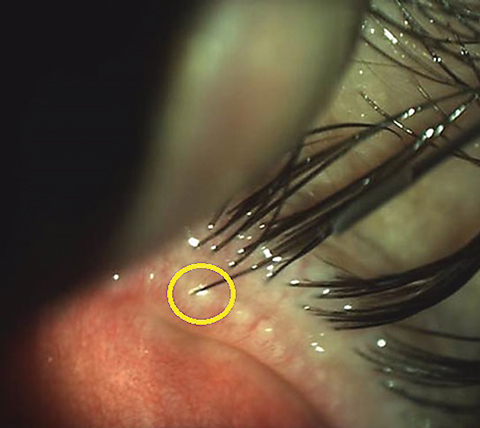 |
| Intraductal meibomian gland probing, a manual procedure to open the meibomian orifices, can be considered in ocular rosacea patients with MGD. Click photo to enlarge. |
While many DED diagnostic tests may be useful, common tests such as the Schirmer’s type 1 test without anesthesia, tear film break-up time (TBUT) and ocular surface vital dye staining may underestimate the presence of DED in patients with Type 2 diabetes.12 Tear osmolarity (Tearlab) may be particularly useful to detect DED in patients with Type 2 diabetes.12 A study comparing tear osmolarity with common DED diagnostic tests in patients with Type 2 diabetes found osmolarity had a greater diagnostic accuracy than Schirmer’s type 1 test, TBUT, rose bengal and fluorescein staining.12
Corneal staining also may be useful in predicting the presence of DED associated with certain systemic diseases. Patients with diabetes are prone to corneal erosions, and one study found corneal sodium fluorescein staining of the inferior corneal zone was predictive of DED in diabetic patients.13,14
 |
| Marked neovascularization of the iris in this patient was caused by uncontrolled proliferative diabetic retinopathy. Click photo to enlarge. Photo: Aaron Bronner, OD |
Customized care. While the current treatment recommendations for diabetic and non-diabetic DED are essentially the same, recent research can guide us in customized treatment plans.
Dietary supplementation with omega-3 fatty acids (FAs), for example, may prevent or even reverse insulin resistance while also improving tear film function and DED symptoms in Type 2 diabetes patients.15-17 The Dry Eye Assessment and Management (DREAM) study—the first large-scale, multicenter, double-masked randomized controlled trial investigating omega-3 FA use for DED—may soon provide a clearer understanding of the efficacy and safety of omega-3 FAs in treating DED. The estimated completion date of the DREAM study is October 2017.18
As chronic hyperglycemia is a risk factor for diabetes-associated DED, patient education on glycemic control is still fundamental, as is education on the chronic nature of their dry eye.5,19 These patients can be asymptomatic, and encouraging both annual ocular surface and fundus evaluations is imperative. Assessment of the retina and the ocular surface should become an integral part of our routine exams when diabetes is suspected.
Referral to an internist, including requests for blood glucose and HbA1c testing, is vital to our management of these patients as well.
Sjögren’s Syndrome
When you suspect a DED patient may have an autoimmune disease, RA, SLE or even sclerodermas are among the conditions on the list. But when a DED patient cites a sore, cracked tongue, one of the most prevalent systemic diseases associated with DED, Sjögren’s syndrome, should move to the top of the list.20
While SS can occur alone in its primary form, about half of SS is found in the presence of another autoimmune connective tissue disease such as RA, and is known as secondary SS.21,22 Immune-mediated damage to the exocrine glands, in particular the lacrimal and the salivary glands, results in the hallmark symptoms of dry eye and dry mouth.22 These and a host of other systemic symptoms can be subtle, episodic and nonspecific, resulting in diagnostic delays.21 Dry eye is often an early symptom, and a timely diagnosis can mitigate serious systemic complications such as lymphoma.
 |
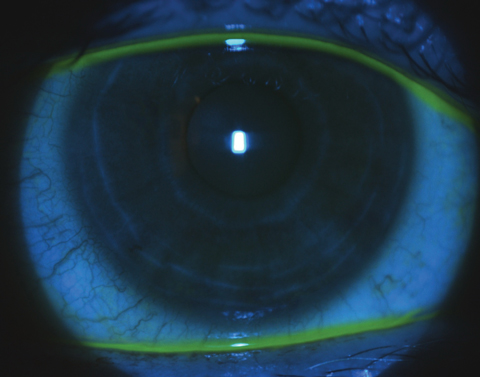 |
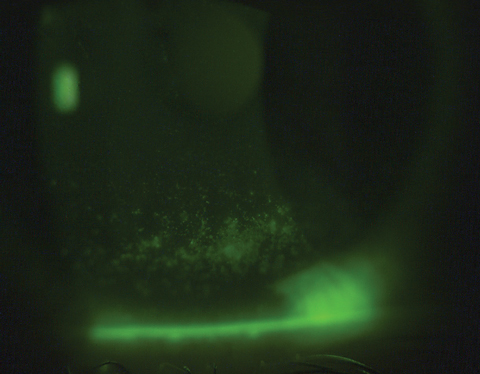
| At top, sodium fluorescein corneal staining of a Sjögren’s syndrome patient prior to scleral contact lens wear. At bottom, reduced sodium fluorescein corneal staining of the same patient three weeks post-scleral lens wear. Click photos to enlarge. |
Clinical clues. To identify SS-associated DED (SS-DED), ask about classic dry eye and dry mouth, as well as prolonged persistent fatigue and joint pain—common SS symptoms.23 Because some classic SS symptoms may not be obvious (a patient may not realize they have dry mouth), clinicians should also explore other nonobvious symptoms such as difficulty talking and swallowing and dental or gum problems.23
As in diabetes-related DED, SS patients may have objective signs of DED without subjective symptoms. A recent study indicates as many as 40% of SS patients with clear objective evidence of DED reported no symptoms.24,25
Important clinical tests in this patient population include ocular vital dye staining and Schirmer’s type 1 testing. The most recently proposed 2016 classification criteria for SS by the American College of Rheumatology/European League Against Rheumatism includes an Ocular Staining Score equal to or greater than five and Schirmer’s type 1 test less than 5mm in five minutes.26
Although SS falls under the umbrella of aqueous-deficient DED, SS patients may have a combination of aqueous-deficient and evaporative DED.4,27 Additionally, ocular surface changes in SS patients may be attributed in part to MGD.28 In a recent study comparing MGD in patients with SS, non-SS dry eye and non-dry eye controls, SS patients had more severe MGD with poorer mean meiboscore and meibomain gland expressibility than non-SS dry eye patients.29
Evaluating DED in patients with SS should include assessment of tear film stability and meibomian gland function. SS-DED may be differentiated from dry eye that is associated with other systemic conditions through various in-office means, such as ocular staining patterns. In one study, researchers showed temporal conjunctival rose bengal staining is a sensitive test for SS and perhaps can be used to differentiate SS-DED from other forms of dry eye.30 Additionally, patchy, central corneal fluorescein staining may also be a good indicator of SS.31
In some states, optometrists can use the Sjö test (Bausch + Lomb), a simple in-office blood test, to diagnose this condition early. Otherwise, patients can be sent to a local laboratory for testing. Referral to a rheumatologist is still advised even when blood tests are negative but symptoms and signs of SS are present. If you or the rheumatologist suspect a false negative test, salivary biopsy may be necessary to confirm the diagnosis.32
Don’t Miss These Often Overlooked AssociationsWhile Type 2 diabetes and Sjögren’s syndrome have a high prevalence in our DED patient population, a variety of other systemic diseases warrant consideration. Graves’ disease. Dry eye is a frequent cause of ocular discomfort in Graves’ disease, a common autoimmune condition.1,2 While the association between Graves’ disease and dry eye is well established, the pathophysiology is not completely understood. The latest evidence points to mechanical impairment of the eyelids, as well as immune-mediated lacrimal gland dysfunction and meibomian gland dysfunction. In a study examining morphologic changes in the meibomian glands of patients with Graves’ orbitopathy compared with controls, a higher prevalence of MGD and more severe dry eye symptoms existed in the Graves’ orbitopathy group than in the control group.3 Multiple sclerosis (MS). This demyelinating disease can lead to severe dry eye. In MS, poor corneal sensory impulse conduction can result in insufficient tear production, and lagophthalmos-associated DED can occur due to poor motor control.4 These patients may have limited ability to instill drops and perform lid hygiene properly; thus, punctal plugs, humidifiers and in-office blepharitis therapies may be crucial. Rosacea. Many patients with cutaneous rosacea cope with ocular symptoms.5 Patients with cutaneous rosacea can develop blepharitis, MGD and associated DED; sometimes, these precede the cutaneous signs. Conventional blepharitis and MGD therapies such as eyelid hygiene and warm compresses, respectively, are mainstay therapies for mild cases. More advanced cases may necessitate topical or oral azithromycin and newer therapies such as intense pulse light and intraductal meibomian gland probing. Rosacea patients should also avoid any triggers such as stress, spicy food, alcohol and excessive sun exposure.6 Pediatric dry eye. Today, we are seeing more DED in children, likely due to the growing use of electronic devices.7 Nonetheless, dry eye in otherwise healthy children is not common and should prompt investigation into a systemic cause such as juvenile RA, juvenile-onset SLE, diabetes, vitamin A deficiency and Riley-Day syndrome.8,9 Systemic medications. While necessary to treat many conditions, pharmaceuticals such as diuretics, antihypertensives, beta-blockers, antidepressants, antipsychotics, antihistamines, decongestants, gastrointestinal medications, oral contraceptives and analgesics may all cause or exacerbate dry eye. Alcohol. The link between DED and alcohol is controversial. One study found that alcohol consumption may be a significant risk factor for dry eye.10 Others suggest alcohol serves a protective role in the development of DED and that drinking and DED may be unrelated.11,12 Based on a meta-analysis of 10 studies, researchers surmise that alcohol-induced peripheral neuropathy may falsely reduce the prevalence of DED.10
|
Customized care. Once the diagnosis is confirmed with a rheumatologist, ODs play a key role in providing customized DED management with new clinical practice guidelines for SS in the United States.33 The recommended DED treatment strategies include both conventional and unconventional therapies such as artificial tears, topical corticosteroids, punctal plugs, autologous serum eye drops (ASEDs) and therapeutic contact lenses.33
Since investigators believe SS-DED is driven by an inflammatory mechanism, anti-inflammatory or immune-modulatory agents are well-suited to treat DED in these patients.34 Research shows Restasis (cyclosporine 0.05%, Allergan) is an effective treatment and may also help SS patients with evaporative DED by treating MGD.35-37
Compounded topical cyclosporine at higher concentrations—including cyclosporine 0.5% to 2% suspension in gum cellulose and cyclosporine 0.2% ointment—may help patients unsuccessful with Restasis.38 Sun Pharma recently announced successful Phase 3 clinical trial results for Seciera (cyclosporine A 0.09% ophthalmic solution).39
Tacrolimus is an another option for SS-DED. In one study, topical 0.03% tacrolimus eye drops improved tear film stability and ocular surface status in SS-related DED.40
Xiidra (lifitegrast ophthalmic solution, Shire) has been successful in randomized, double-masked, multicenter, placebo-controlled studies in improving DED symptoms and signs—promising results for SS patients.41
Omega-3 FA supplementation is also a good anti-inflammatory management option. However, high intake of omega-3 FAs can cause excessive bleeding in some patients, and patients should take then under a physician’s care.25
Although SS patients are treated with Plaquenil (hydroxychloroquine, Sanofi-Aventis) systemically, it is known to cause retinopathy and its benefit for SS-DED is controversial.42,43,44 While research shows Plaquenil improves dry eye in primary Sjögren’s subjects, other studies show no clinical benefit.42,43 Clinicians should follow the 2016 updated visual screening guidelines for long-term Plaquenil therapy.44
The secretagogues oral pilocarpine and cevimeline are indicated for dry mouth in SS patients, but their benefit for SS-DED is controversial.31 While some research shows they improve DED symptoms and signs, others show they were ineffective in improving DED signs.25
Recently, scleral gas permeable lenses have gained attention for their success in treating SS-DED. Although no studies specifically investigate the outcomes of scleral lenses in patients with SS, these patients have been included in several study groups and have benefited from scleral lenses.45-47 Anecdotally, practitioners find SS patients have improved symptoms and signs with scleral lenses and indicate a significant improved quality of life.
SS-DED can be severe, and other therapies typically reserved for refractory DED such as sutureless amniotic membranes and autologous serum drops may be helpful for these patients. Sutureless amniotic membranes act as bandage and restore the epithelium and control inflammation.48 ASEDs also promote epithelialization and can be an effective DED treatment for SS patients.49-51 Punctal plugs combined with ASEDs may have an additive effect and perhaps should be considered in recalcitrant cases after using ASEDs alone.51
Dry eye disease is associated with several systemic diseases with serious complications. Fortunately, optometrists are in a vital position to address these patients’ dry eye needs and manage their holistic health approach.
Dr. Mickles is associate professor at Nova Southeastern University College of Optometry and its Dry Eye Service coordinator. She is a fellow of the American Academy of Optometry.
| 1. Centers for Disease Control and Prevention. Increasing prevalence of diagnosed diabetes-United States and Puerto Rico, 1995-2010. Morb Mortal Wkly Rep. 2012;61(45):918-21. 2. Lerner A, Jeremias P, Matthias T. The world incidence and prevalence of autoimmune diseases is increasing. Internat J Celiac Disease. 2015;3(4):151-5. 3. Kruszka P, O’Brian RJ. Diagnosis and management of Sjögren syndrome. Am Fam Physician. 2009;79(6):465-70. 4. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop. Ocul Surf. 2007;5:75–92. 5. Zhang X, Zhao L, Deng S, et al. Dry eye syndrome in patients with diabetes mellitus: Prevalence, etiology, and clinical characteristics. J Ophthalmol. March 2016. [Epub]. 6. Manviat M, Rashidi M, Afkhami-Ardekani M, Shjoa MR. Prevalence of dry eye syndrome and diabetic retinopathy in type 2 diabetic patient. BMC Ophthalmology. 2008;8(10). 7. Nepp C, Abela I, Polzer A, et al. Is there a correlation between the severity of diabetic retinopathy and keratoconjunctivitis sicca? Cornea. 2000;19(4):487-91. 8. Hom M, De Land P. Self-reported dry eyes and diabetic history. Optometry. 2006;77(11):554-8. 9. Kaiserman I, Kaiserman N, Nakar S, Vinker S. Dry eye in diabetic patients. Am J Ophthalmol. 2005;139:498-503. 10. Garzon Johanna P, Lopez-Alemany A. Clinical features of meibomian gland dysfunction in patients with diabetes Type 2. Poster presented at the 8th International TFOS Conference, September 7-10, 2016, Montpellier, France. 11. Shamsheer RP, Arunachalam C. A clinical study of meibomian gland dysfunction in patients with diabetes. Mid East Afr J Ophthalmol. 2015;22(4):462-6. 12. Najafi L, Malek M, Valojerdi AE, et al. Dry eye disease in type 2 diabetes mellitus; comparison of the tear osmolarity test with other common diagnostic tests: a diagnostic accuracy study using STARD standard. J Diabetes Metab Disord. 2015;14:39. 13. Fenner BJ, Tong L. Corneal staining characteristics in limited zones compared with whole cornea documentation for the detection of dry eye subtypes. Invest Ophthalmol Vis Sci. 2013;54(13):8013-9. 14. Rosenberg ME, Tervo TM, Immonen IJ, et al. Corneal structure and sensitivity in type 1 diabetes mellitus. Invest Ophthalmol Vis Sci. 2000;41(10):2915-21. 15. Davi G, Santilli F, Patrono C. Nutraceuticals in diabetes and metabolic syndrome. Cardiovasc Ther. 2010;28:216-26. 16. Fedor D, Kelley DS. Prevention of insulin resistance by n-3 polyunsaturated fatty acids. Curr Opin Clin Nutr Metab Care. 2009;12:138–46. 17. Georgakopoulos CD, Makri OE, Pagoulatos D. Effect of omega-3 fatty acids dietary supplementation on ocular surface and tear film in diabetic patients with dry eye. J Am Coll Nutr. 2017;36(1):38-43. 18. Dry Eye Assessment and Management Study (DREAM). clinicaltrials.gov/ct2/show/NCT02128763. Accessed July 13, 2017. 19. Seifart U, Strempel I. The dry eye and diabetes mellitus. Ophthalmologe. 1994;91(2):235-9. 20. Henrich CF, Ramulu PY, Akpek EK. Association of dry eye and inflammatory systemic diseases in a tertiary care-based sample. Cornea. 2014;33(8):819-25. 21. Beckman KA, Luchs J, Milner MS, Ambrus JL Jr. The potential role for early biomarker testing as part of a modern, multidisciplinary approach to Sjögren’s syndrome diagnosis. Adv Ther. 2017;34(4):799-12. 22. Canellos HM. Sjögren’s syndrome. In: Marks ES, Adamcyzk DT, Thomann KH, eds. Primary Eyecare in Systemic Disease. 2nd ed. New York, NY: McGraw-Hill 2001:311-7. 23. Birnbaum J. Peripheral nervous system manifestations of Sjögren syndrome: clinical patterns, diagnostic paradigms, etiopathogenesis, and therapeutic strategies. Neurologist. 2010;16(5):287-97. 24. Sullivan BD, Crews LA, Messmer EM, et al. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: clinical implications. Acta Ophthalmol. 2014;92:161-6. 25. Foulks GN, Forstot SL, Donshik PC, et al. Clinical guidelines for management of dry eye associated with Sjögren disease. Ocul Surf. 2015;13(2):118-32. 26. Shiboski CI, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism classification fcriteria for primary Sjogren’s syndrome: A consensus and data-driven methology involving three international patient cohorts. Ann Rheum Dis. 2017 Jan;76(1):9-16. 27. Akpek EK, Klimava A, Thorne JE, et al. Evaluation of patients with dry eye for presence of underlying Sjögren syndrome. Cornea. 2009;28(5):493-7. 28. Shimazaki J, Goto E, Ono M, et al. Meibomian gland dysfunction in patients with Sjögren syndrome. Opthalmology. 1998;105(8):1485-8. 29. Kang YS, Lee HS, Li Y, et al. Manifestation of meibomian gland dysfunction in patients with Sjogren’s syndrome, non-Sjogren’s dry eye, and non-dry eye controls. Int Ophthalmol. 2017 May 31:1-7. 30. Caffery B, Simpson T, Wang S, et al. Rose Bengal staining of the temporal conjunctiva differentiates Sjögren’s syndrome from keratoconjunctivitis sicca. Invest Ophthalmol Vis Sci. 2010 May;51:2381-7. 31. Cunningham DN, Nichols K, Karpecki P, Devries D. Frontline ocular surface disease care. Rev Optom. 2017;154(3):29-35. 32. Sheldon J. Laboratory testing in autoimmune rheumatic diseases. Best Pract Res Clin Rheumato. 2004;18(3):249-69. 33. Vivino FB, Carson SE, Foulks G, et al. New treatment guidelines for Sjögren’s disease. Rheum Dis Clin North Am. 2016;42(3):531-51. 34. Baudouin C. The pathology of dry eye. Surv Ophthalmol. 2001;45(Suppl 2):S211-20. 35. Baudouin C, Pisella PJ, Brignole F. Current treatments of xerophthalmia in Sjögren’s syndrome Rev Med Interne. 2004 May;25(5):376-82. 36. Perry HD, Doshi-Carnevale S, Donnenfeld ED, et al. Efficacy of commercially available topical cyclosporine A 0.05% in the treatment of meibomian gand dysfunction. Cornea. 2006;25:171-5. 37. Rubin M, Rao SN. Efficacy of topical cyclosporine 0.05% in the treatment of posterior blepharitis. J Ocul Pharmacol Ther. 2006;22(1):47–53. 38. Kabat AG. Customized solutions for the dry eye patient. Rev Optom. 2015;152(1):100. 39. Sun Pharma. Sun pharma announces positive topline results of confirmatory phase-3 clinical trial for seciera for treatment of dry eye. January 4, 2017. www.sunpharma.com/media/press-releases. Accessed July 12, 2017. 40. Moscovici BK, Holzchuh R,Sakassegawa-Naves FE, et al. Treatment of Sjögren’s syndrome dry eye using 0.03% tacrolimus eye drop: Prospective double-blind randomized study. Cont Lens Anterior Eye. 2015;38(5):373-8. 41. Holland EJ, Luchs J, Karpecki PM, et al. Lifitegrast for the treatment of dry eye disease: Results of a phase III, randomized, double-Masked, placebo-Controlled Trial (OPUS-3). Ophthalmology. 2017;124(1):53-60. 42. Yavuz S, Asfouroglu, E, Bicakcigil M, Toker E. Hydroxychloroquine improves dry eye symptoms of patients with primary Sjogren’s syndrome. Rheumatol Int. 2011;31(8):1045-9. 43. Yoon CH, Lee HJ, Lee EY, et al. Effect of hydroxychloroquine treatment on dry eyes in subjects with primary Sjogren’s syndrome: A double-blind randomized control study. J Korean Med Sci. 2016 Jul; 31(7):1127-35. 44. Marmor MF, Kellner U, Lai TY, et al. Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy (2016 Revision). Ophthalmology. 2016;123(6):1386-94. 45. Weber SL, de Souza RB, Gomes JÁ, Hofling-Lima AL. The use of the esclera scleral contact lens in the treatment of moderate to severe dry eye disease. Am J Ophthalmol. 2016; 163:167-73.e1. 46. Alipour F, Kheirkhah A, Behrouz M. Use of mini-scleral contact lenses in moderate to severe dry eye. Cont Lens Anterior Eye. 2012;35(6):272-6. 47. Schornack M, Pyle J, and Patel S. Scleral lenses in the management of ocular surface disease. Ophthalmology. 2014; 21:1398-1405. 48. Suri K, Kosker M, Raber IM, et al. Sutureless amniotic membreane Prokera for ocular surface disorders: short term results. Eye Contact Lens. 2013;39 (5):341-7. 49. Tsubota K, Goto E, Fujita H, et al. Treatment of dry eye by autologous serum application in Sjogren’s syndrome. Br J Ophthalmol. 1999;83: 390–5. 50. Kojima T, Ishida R, Dogru M, et al. The effect of autologous serum eye drops in the treatment of severe dry eye disease: a prospective randomized case-control study. Am J Ophthalmol. 2005; 39:242–6. 51. Liu Y, Hirayama M, Cui X, Connell S et al. Effectiveness of autologous serum eye drops combined with punctal plugs for the treatment of Sjogren;s syndrome-related dry eye. Cornea 2015;34 (10):1214-20. |
